

Today, we would like to introduce the challenging supraarchal branch in situ reconstruction TEVAR surgery brought by the team of Professor Fu Weiguo from Zhongshan Hospital Affiliated to Fudan University. The case was a bovine aortic arch with a large aneurysm lesion located in the anterior wall of the aortic arch, proximal involvement of the root of the left subclavian artery, and stenosis of the left subclavian artery opening. Thoracoabdominal aortic atherosclerosis, multiple mild to moderate stenosis, and left renal artery stenosis. The surgical team, together with Prof. Yang Jue, Prof. Zhu Ting and Dr. Pan Tianyue, successfully performed in situ reconstruction of the left subclavian artery using only 0.018" CTO guidewire soft head to instantly penetrate the graft.
Description
Gender: Male
Age: 69 years old
History of present illness: 3 months ago, due to abnormal elevation of body temperature, CTA of the hospital showed abdominal aortic aneurysm.
Anamnesis: 4 months ago, he had undergone "choletomy" in the outer hospital due to cholecystitis.
Preoperative diagnosis: aortic arch aneurysm, renal artery stenosis, abdominal aortic dissection.
CTA Explained:
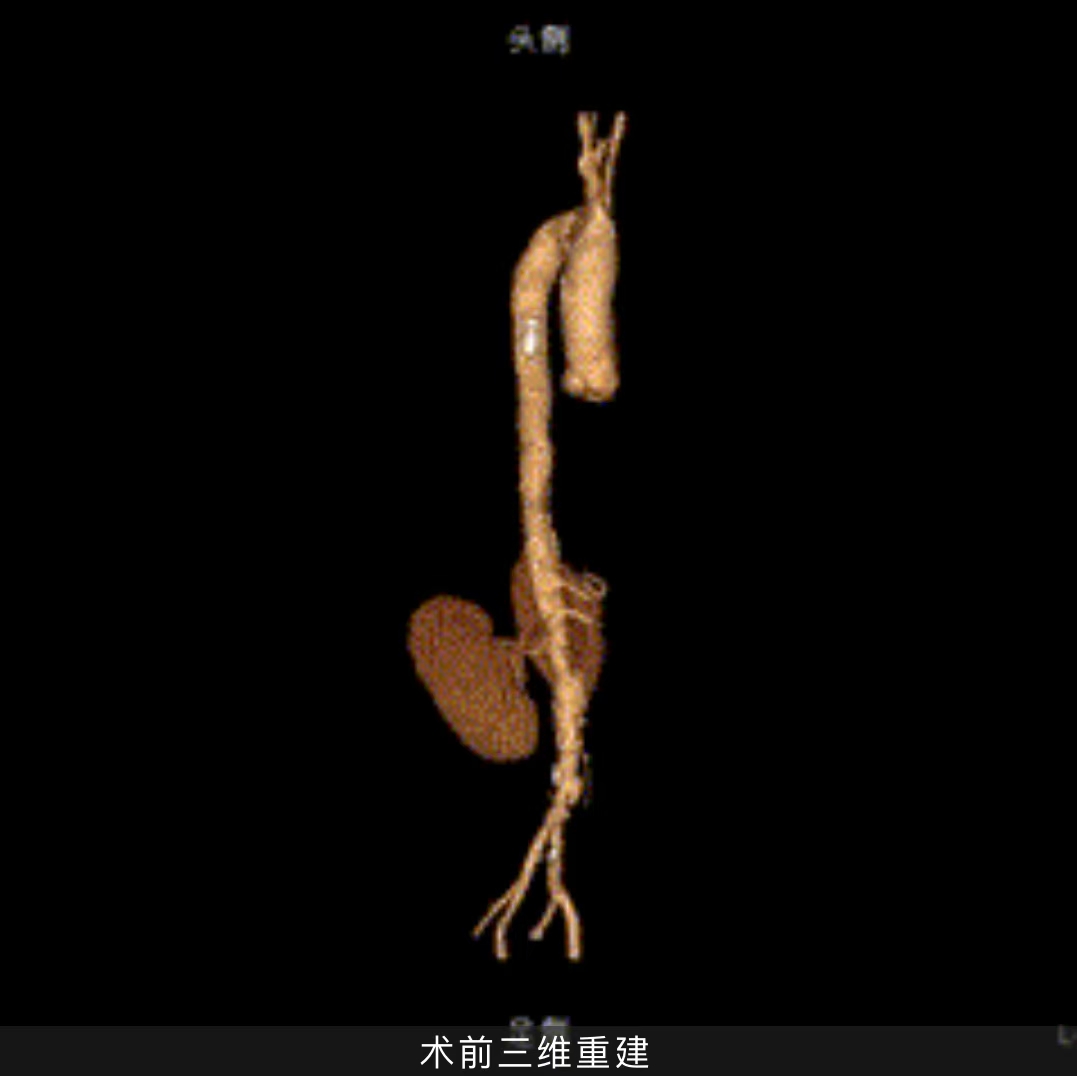
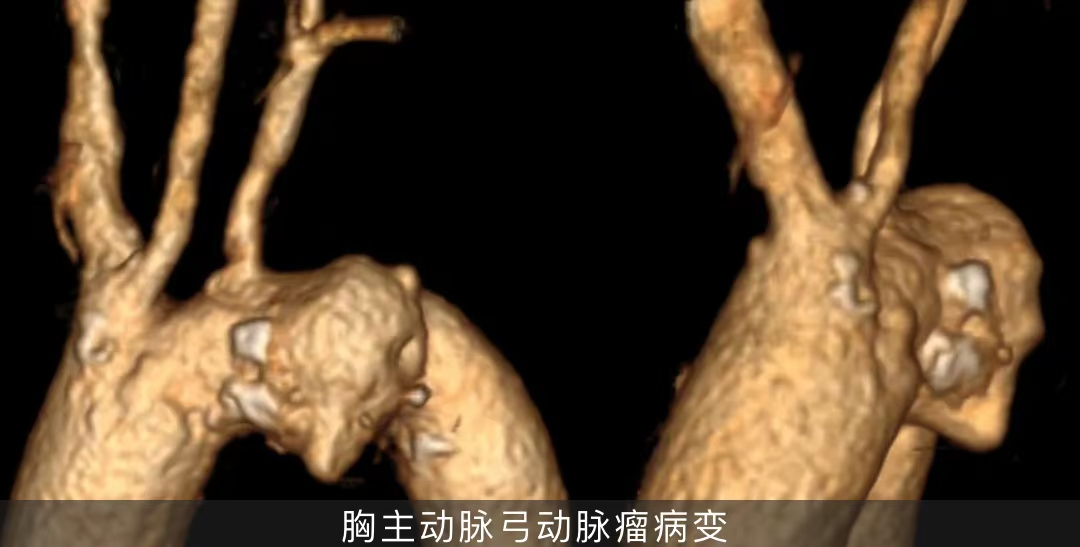
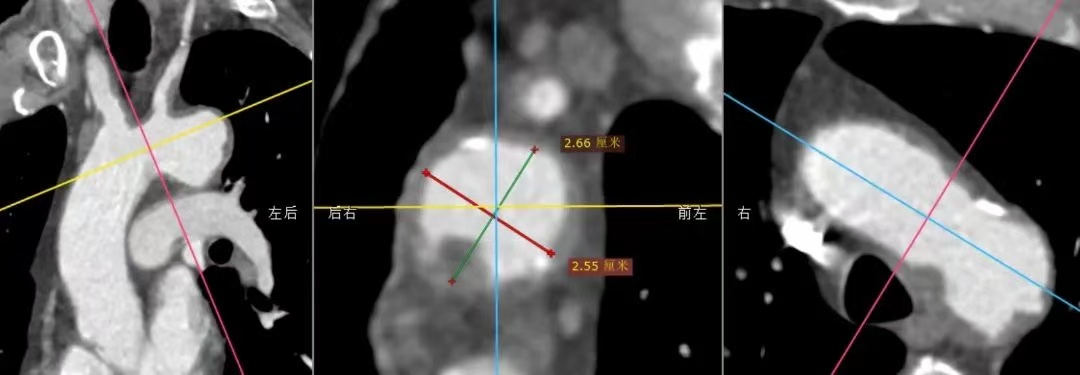
thoracic aortic arch aneurysm, the lesion is located in the anterior wall, the aneurysm size is 43*35*12mm, the proximal end involves the proximal end of the left subclavian artery, and the left subclavian artery opening is narrowed; Bovine arch with a distal brachiocephalic artery only 11 mm proximal to the left subclavian artery. The diameter of the aorta at the neck of the aneurysm is 26.6*25.5mm. Thoracoabdominal aortic atherosclerosis with multiple mild to moderate stenosis of the lumen, multiple ulcers and multiple calcifications of the wall, and local penetrating ulcer of the lower abdominal aorta with localized dissection. Mild stenosis of the superior mesenteric artery, moderate to severe stenosis of the initial segment of the left renal artery, and cyst of the left kidney.


Difficult to operate
•The proximal end of the thoracic aortic arch aneurysm has involved the root of the left subclavian artery, and the proximal anchoring area is markedly insufficient.
•Large aneurysm lesions require high proximal sealing of thoracic aortic stent grafts.
•The left subclavian artery originates from the posterior wall of the aortic arch and is stenosis at the opening, which makes it difficult to control the angle of in-situ fenestration during surgery.
•Thoracoabdominal aortic atherosclerosis, multiple mild to moderate stenosis, and certain requirements for the passage of the thoracic aortic stent graft delivery system.
•Multiple calcifications in the aortic arch should be exercised gently.
Surgical protocol strategy
01. Thoracic aortic stent graft endovascular repair directly covering the left subclavian artery: the operation is simple and the effect is clear, but covering the left subclavian artery may bring clinical manifestations of posterior circulation ischemia and upper limb ischemia to patients.
02. Thoracic aortic stent graft endovascular repair + left subclavian artery chimney technique: the surgical operation is relatively simple, but the left subclavian artery is stenosis, the risk of endoleakage and occlusion is greater, and the medium and long-term effect is not good.
03. Endovascular repair of thoracic aortic stent graft under external fenestration: thoracic aortic aneurysm closure effect is good, and the original hemodynamic characteristics can be retained, but the operation is complicated, and the stent needs to be modified according to the measurement results before surgery, which takes a long time; Intraoperative hyperselection windows require precise alignment, which is a high risk.
04. Single-branch stent thoracic aortic endovascular repair: the closure effect of thoracic aortic aneurysm is good, but the angle between the left subclavian artery and the aortic arch is too small, and the left subclavian artery is occluded proximally, and the risk of long-term occlusion of the branch stent increases.
05. Thoracic aortic stent graft endovascular repair + in-situ fenestration: the lesion closure effect is good, and there is no need to modify the stent before surgery. However, the in-situ fenestration of traditional aortic stent grafts has high requirements for interventional devices, and special membrane permeation instruments such as in-situ fenestration needles, lasers, and biopsy needles are required.
Considering the medium- and long-term treatment effect and the simplicity of intraoperative operation, we again selected HuamaiTech thoracic aortic stent graft for endovascular repair and in-situ fenestration to reconstruct the left subclavian artery.
Surgical procedure
Thoracic aortic branch stent grafting + subclavian ball dilation stent placement + renal glomerulum stent placement + thoracic aortography + renal arteriography
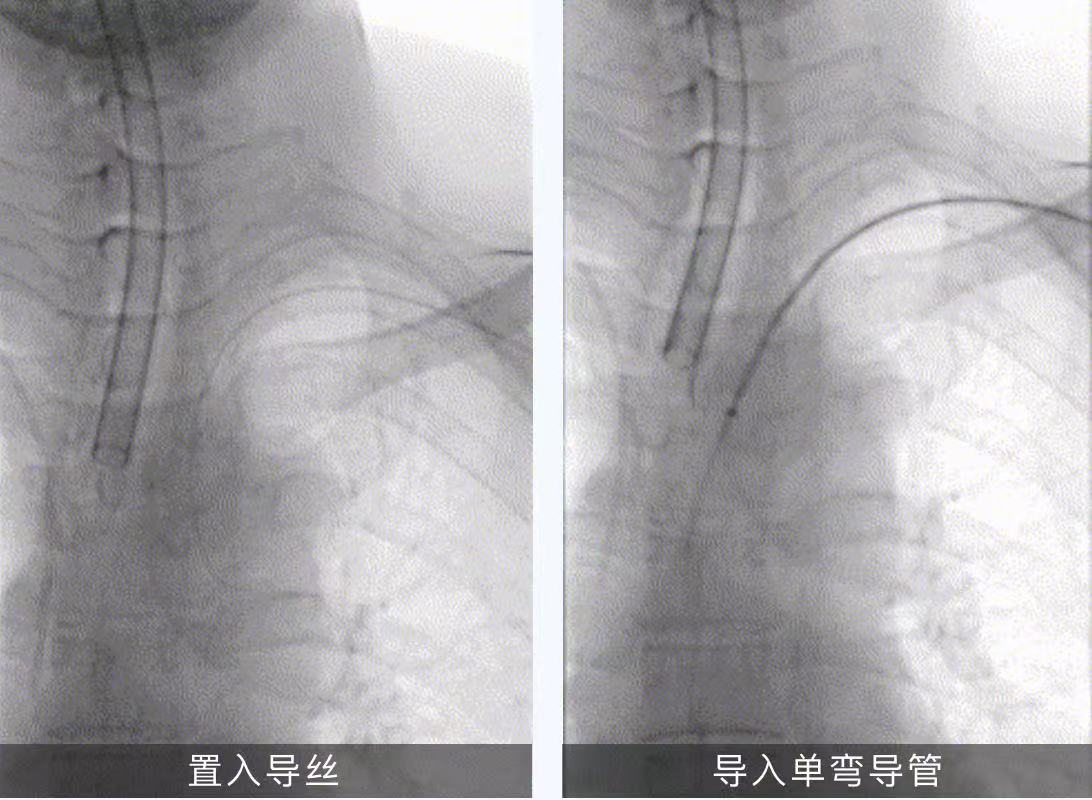
01. Supine position, conventional sterilization and drape, left upper limb incision, separation of the brachial artery, placement of the 5F sheath, selection of the guidewire catheter into the aortic arch, exchange of Amplatz hard guidewire, placement of the 7F long sheath. The left femoral artery was punctured, a 5F sheath was inserted, 2 staplers were preset, a loach guidewire and a pigtail catheter were introduced, the guidewire catheter was selected into the ascending aorta, a single-bent catheter and a loach guidewire were introduced, and Lunderquist super-rigid guidewires were exchanged.
02. Angiography: aortic arch ulcer with aneurysm, involving the proximal left subclavian artery.
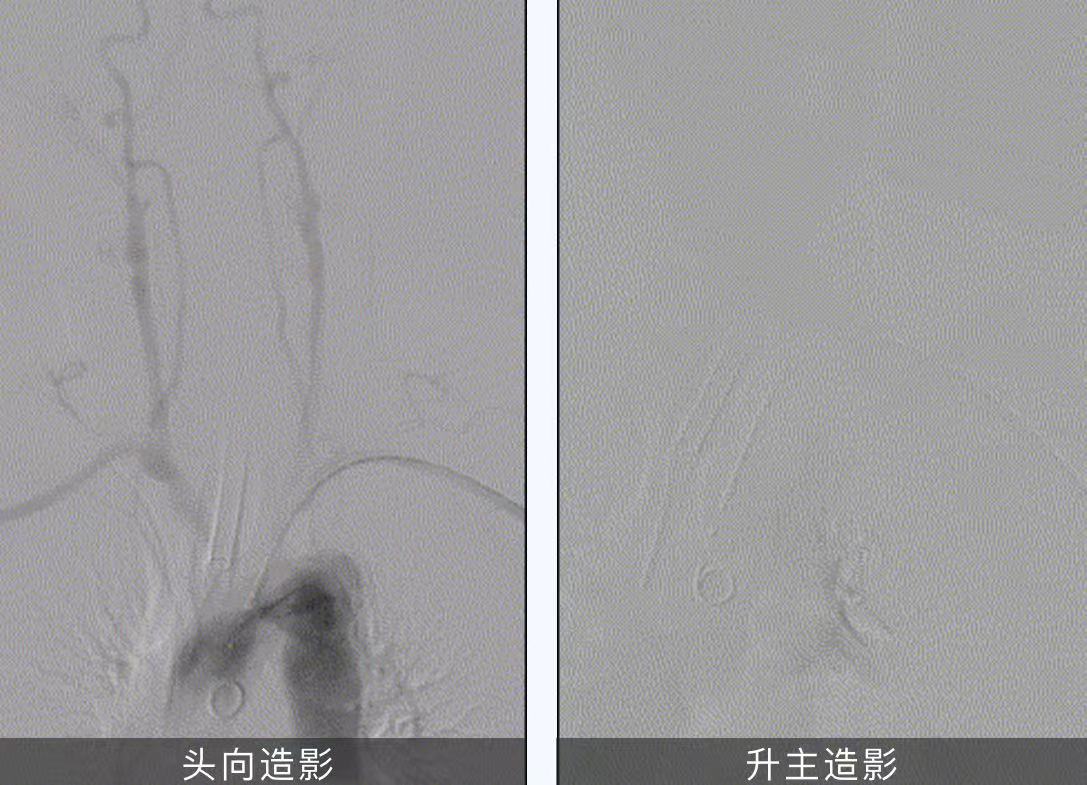
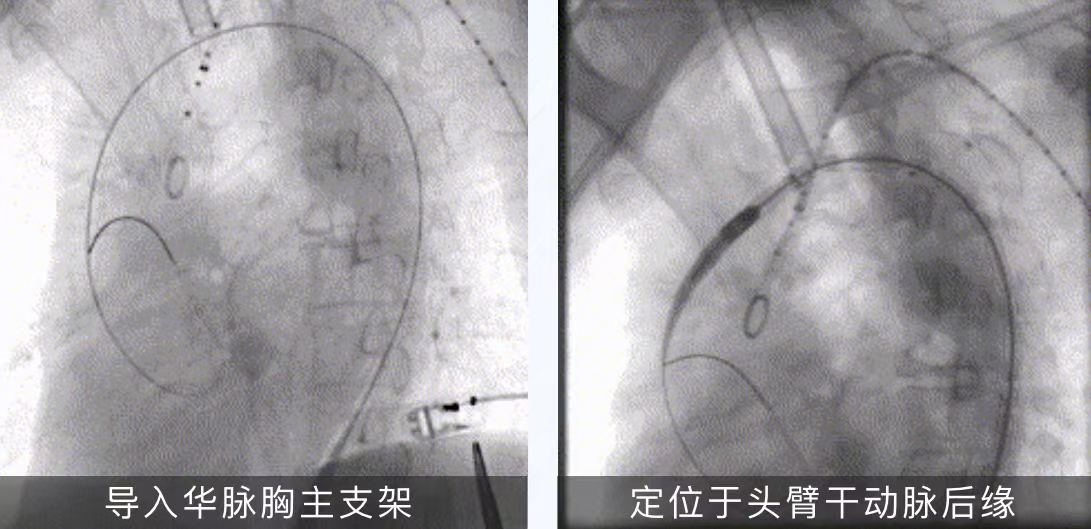
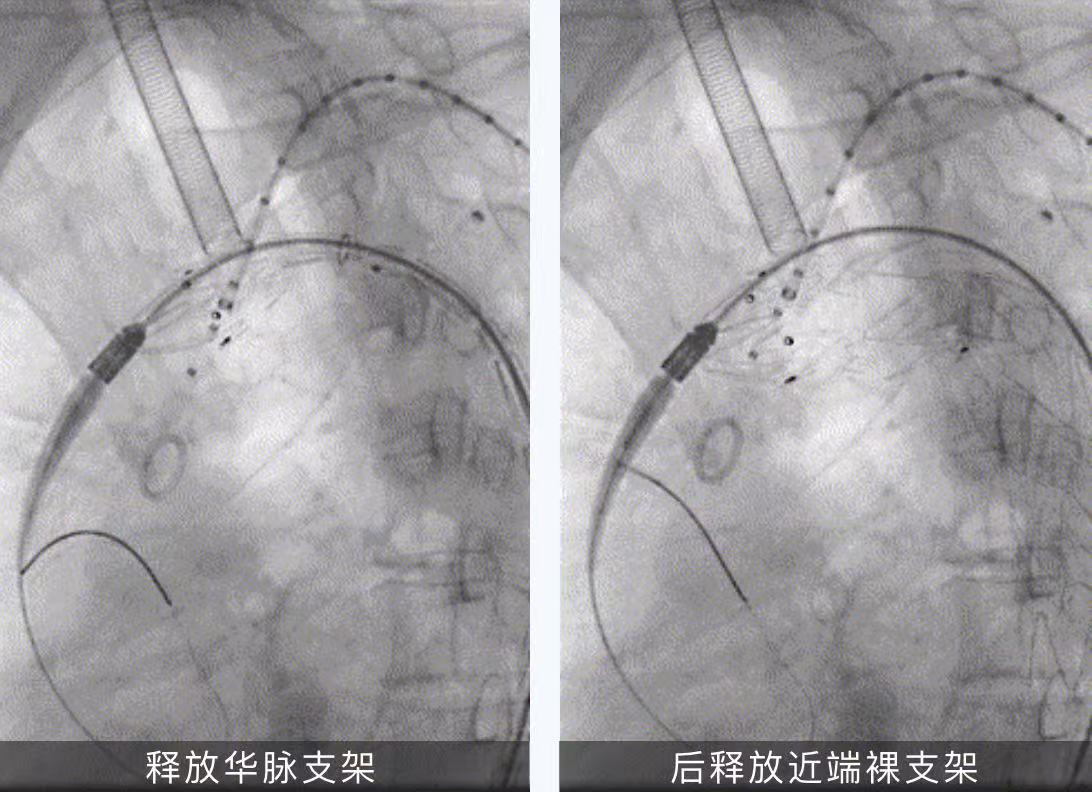
03. Introduced Huamai Tianyi ® thoracic aortic stent graft PTBS3026180, and the proximal end was positioned at the posterior edge of the brachiocephalic artery for release.
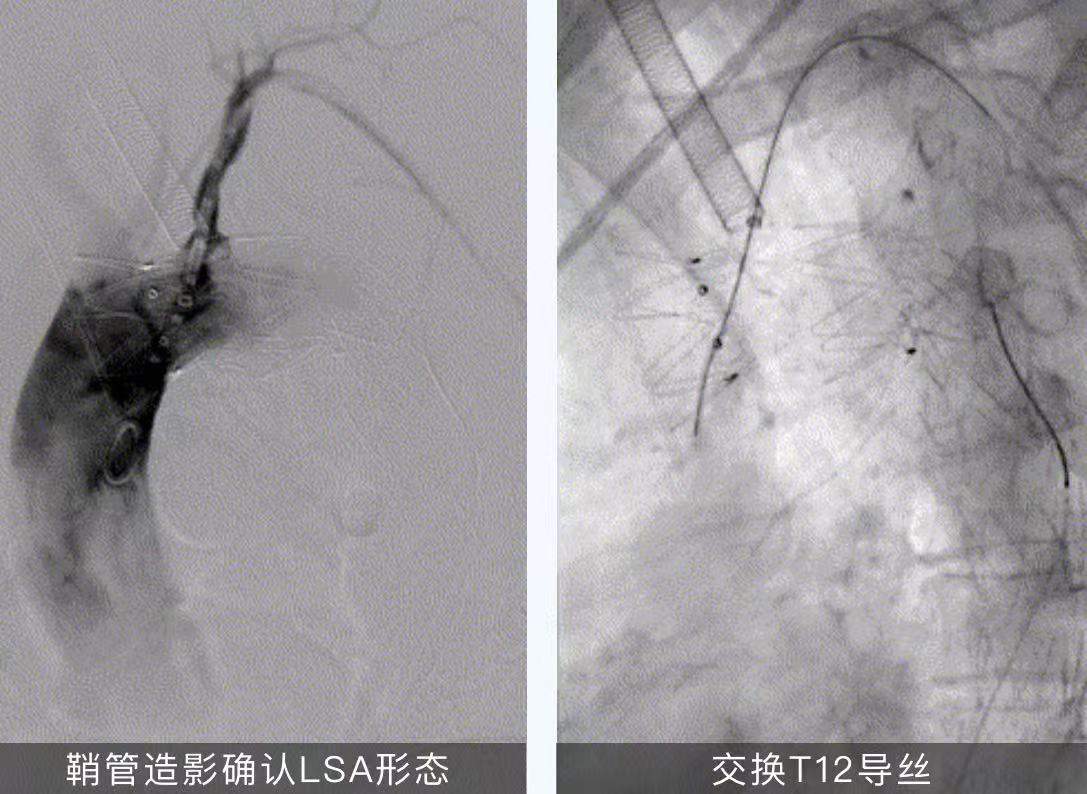
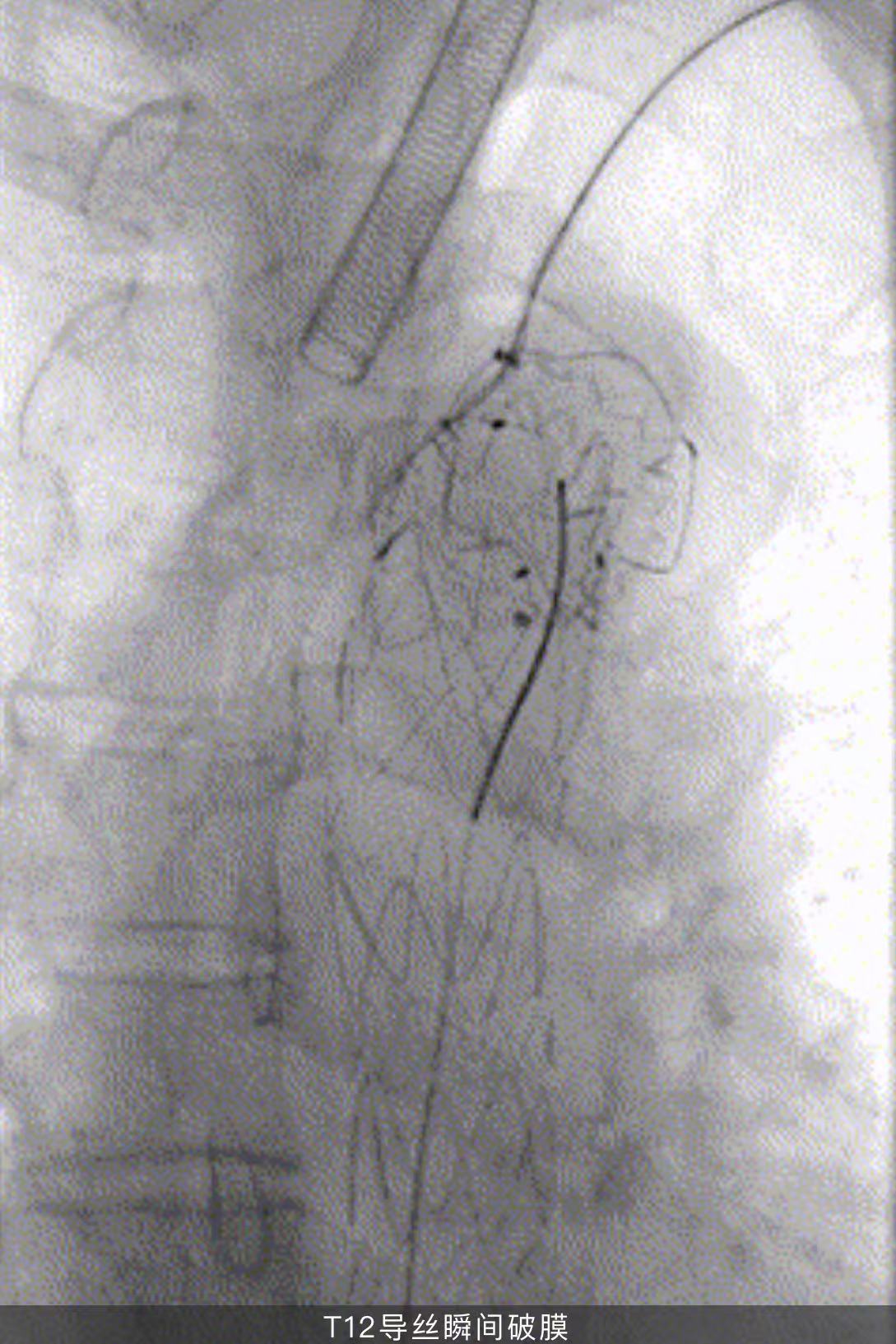
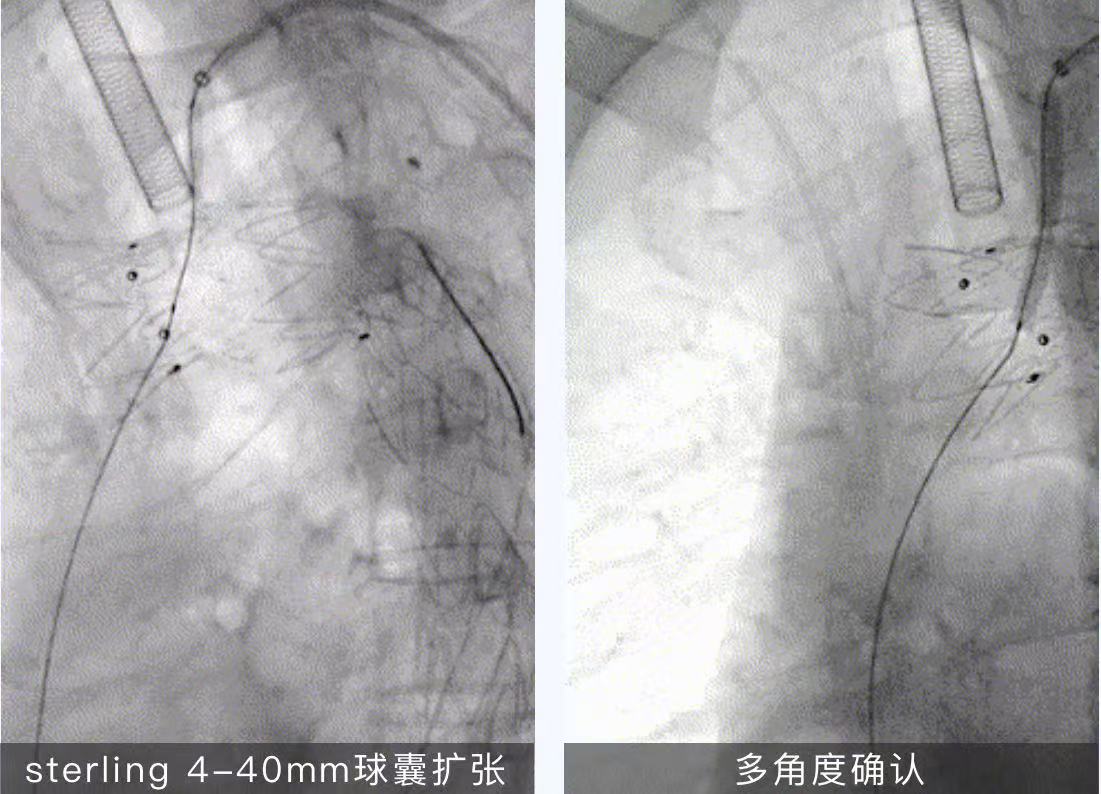
04. Use a T12 guidewire with a single-bent catheter to penetrate the aortic stent graft and enter the ascending aorta, and then use a sterling 4-40mm balloon and a Mustang 6-40mm balloon to dilate the window.
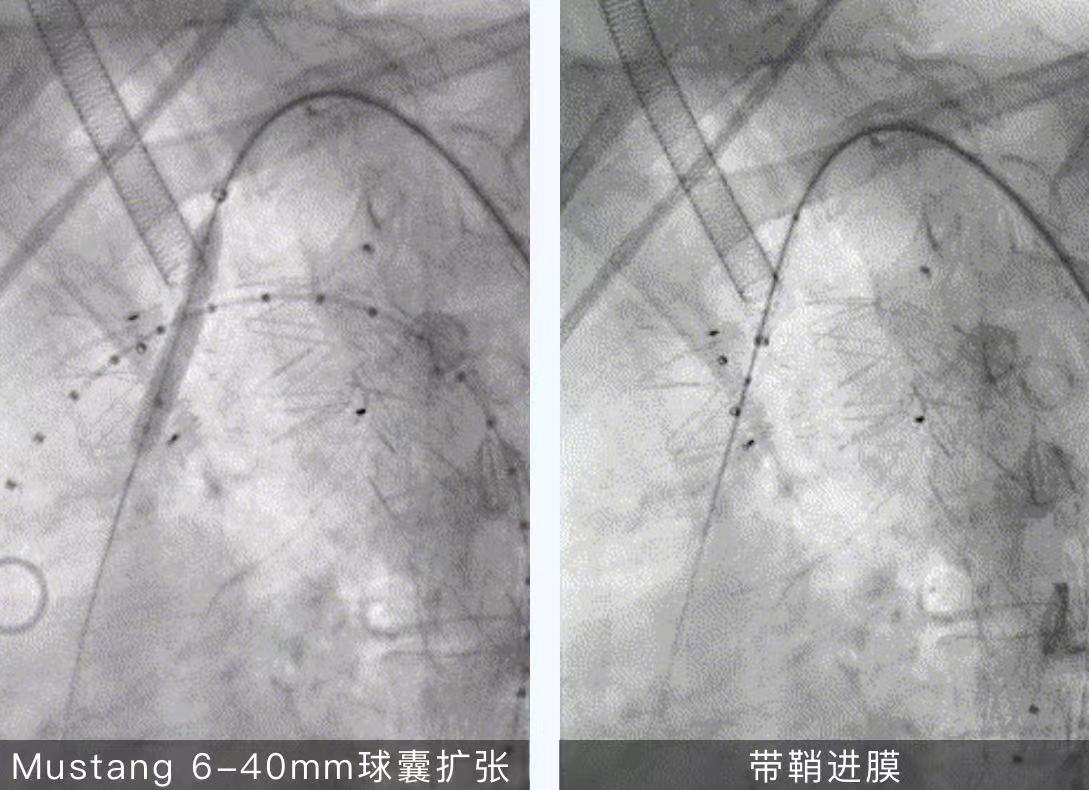
05. Swap the Amplatz hard guidewire and introduce the 8-39mm VBX spherical expansion stent to position the left subclavian artery dilation release.
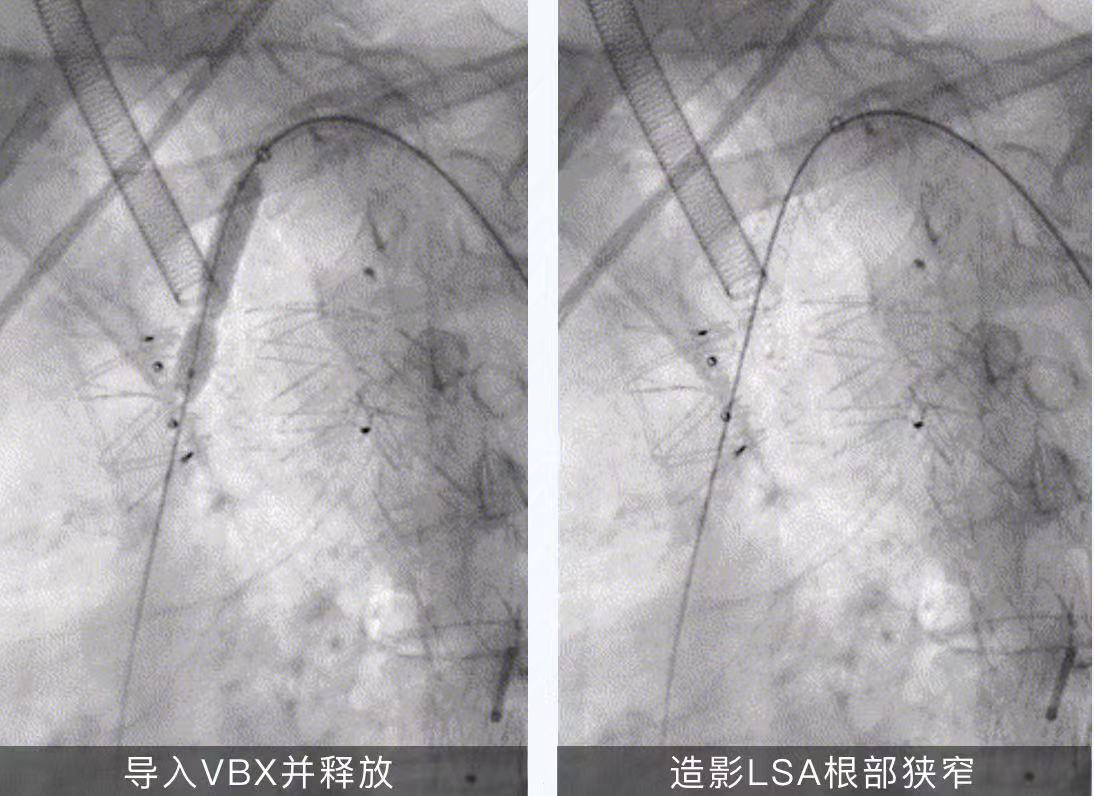
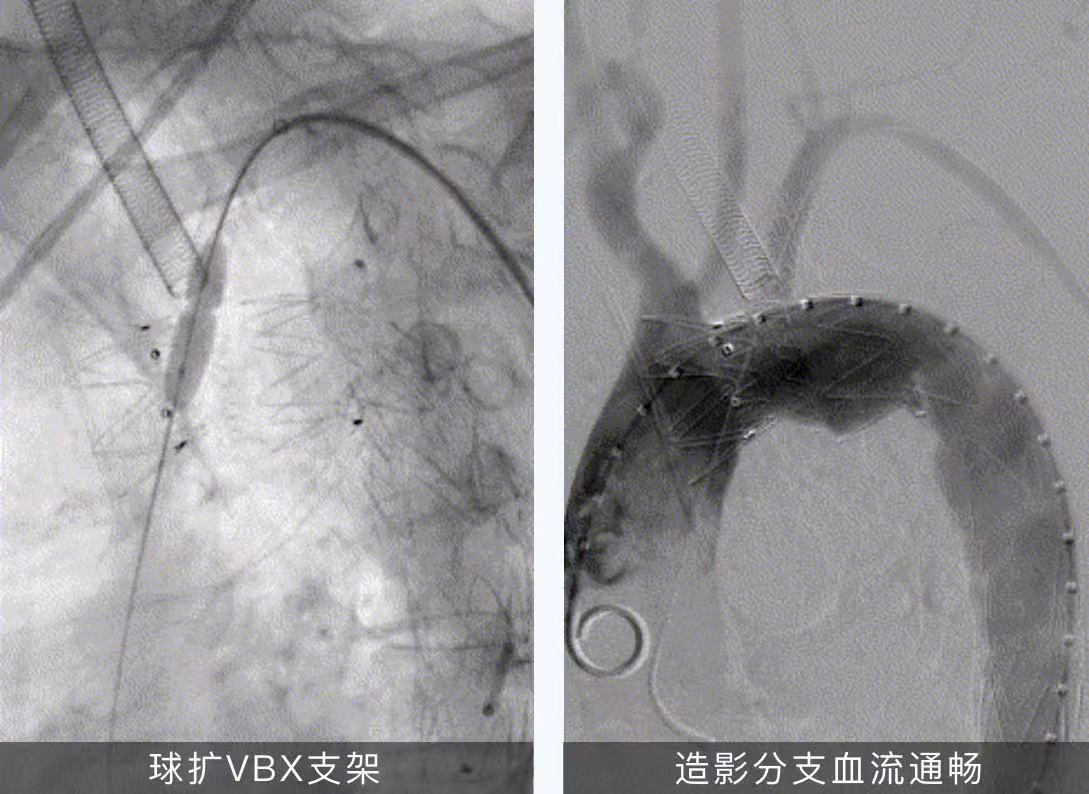
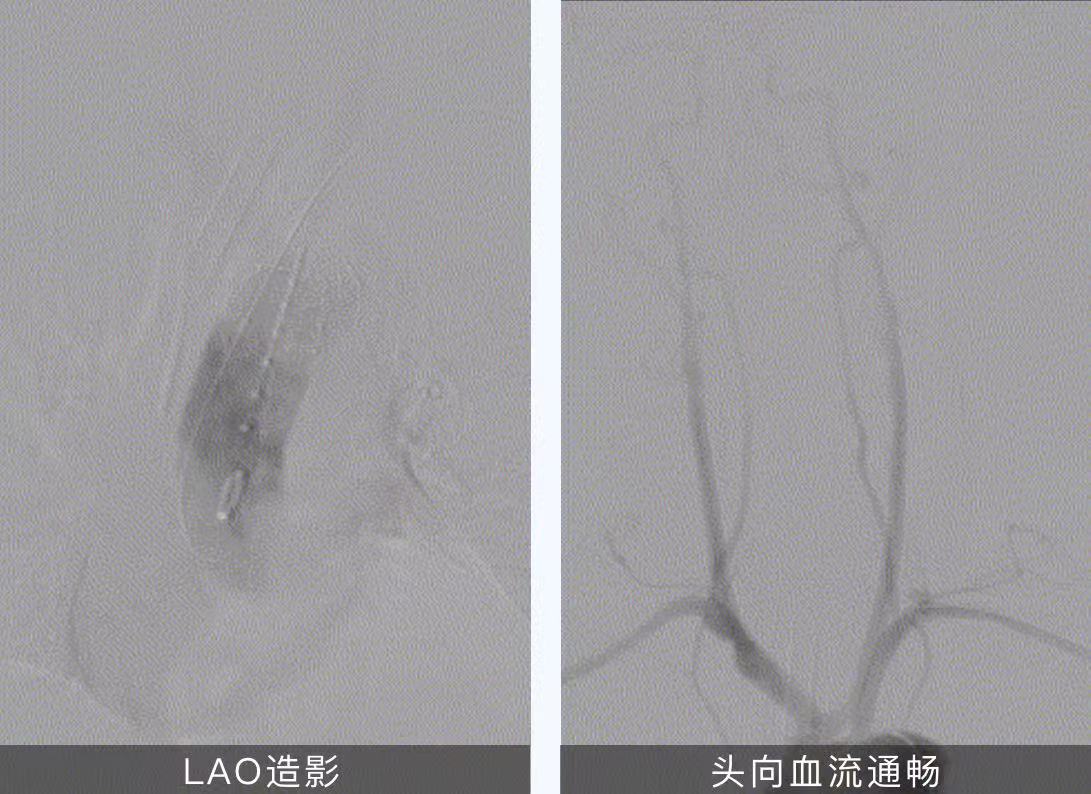
06. Angiography: smooth blood flow in the aortic stent, no obvious endoleakage, no development of the original aneurysm cavity, smooth blood flow in the branch stent above the aortic arch, positive blood flow in the left subclavian artery, good imaging of bilateral carotid arteries and vertebral arteries, and good visualization of intracranial arteries.
07. Catheter into abdominal aortogram: left renal artery proximal stenosis, right renal artery blood flow is smooth, C2 catheter and V18 guidewire are introduced into the left renal artery, expressSD 5-19mm balloon dilation stent is introduced and dilated, contrast: blood flow in the renal artery stent is smooth, and there is no obvious exudation from the left kidney.
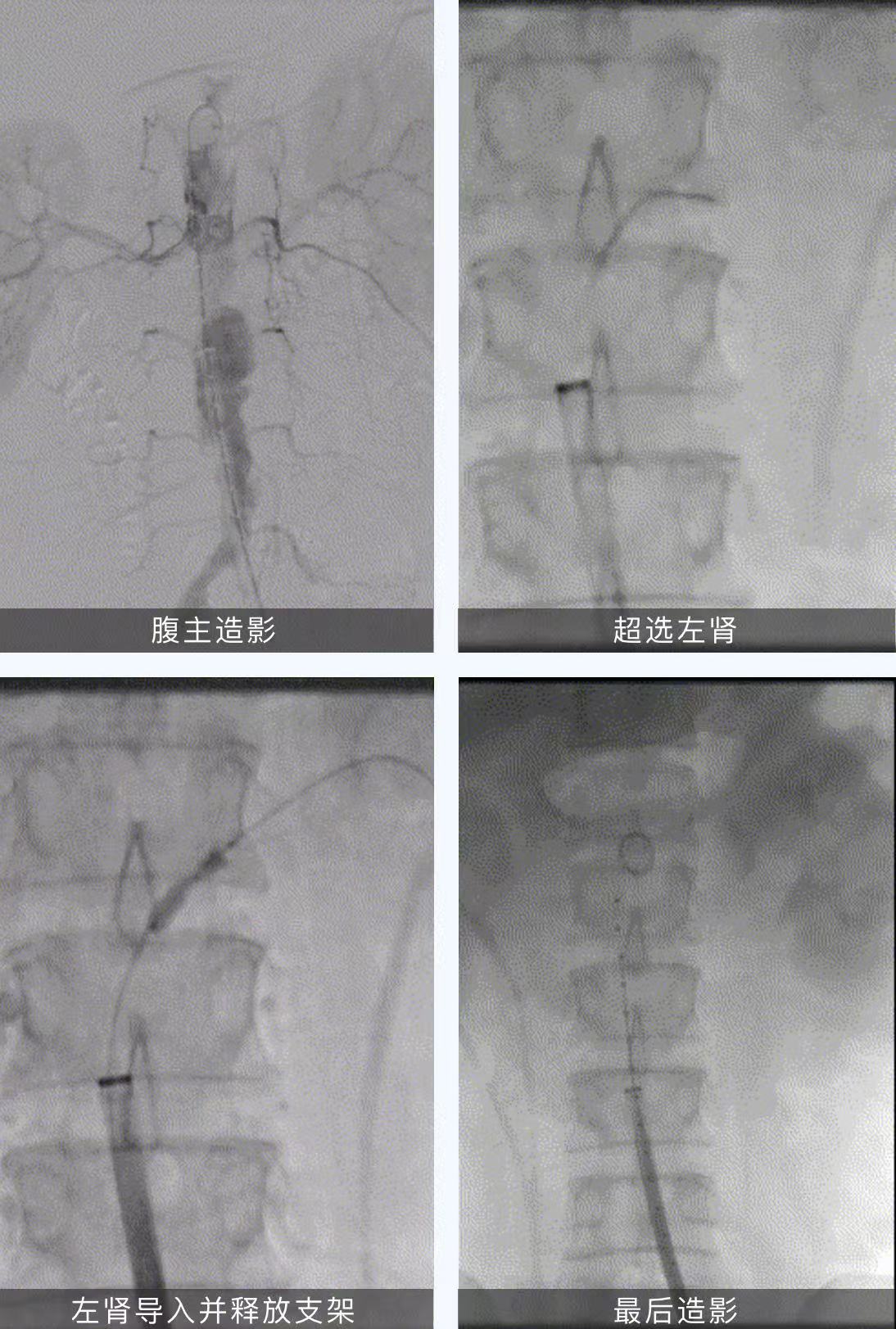
08. Exit the guidewire, catheter, and sheath. Suture the puncture point and close the skin. Completion of the operation.
Summary of case lessons
In this case, the patient is a bovine aortic arch with a large aneurysm lesion, located in the anterior wall of the aortic arch, the proximal end has involved the root of the left subclavian artery, the proximal anchoring area is insufficient, and the left subclavian artery opening is narrow. While expanding the anchoring area and ensuring the medium- and long-term treatment effect of patients, we chose to reconstruct the left subclavian artery through in-situ fenestration technology, which ultimately ensured the effect of lesion closure and ensured the perfusion of blood flow in the left subclavian artery. In addition, the patient had multiple mild to moderate stenosis and multiple calcifications of the thoracic and abdominal aorta, which required high proximal sealing, overall compliance and adhesion of the thoracic aortic stent graft.
Huamai Tech's thoracic aortic stent graft performed well in the process of in-situ reconstruction of the supraarch branch, the proximal positioning of the stent graft was accurate, there was no endoleakage, the membrane could be broken instantaneously with only 0.018" T12 CTO guidewire soft head during the operation, the lamination at the window opening was easy to penetrate and expand, the balloon dilation opening process was simple, safe and reliable, and the selection requirements for intracavity equipment were reduced, and the whole operation took only 50 minutes from the first imaging to the last imaging. After stent implantation, the shape was good, there was no membrane leakage, the effect was clear, and the prognosis of the patient was good, and finally the reconstruction effect of the left subclavian artery in this case was in line with the preoperative planning expectations.
