Subclavian artery stenosis has been attracting attention in recent years because it is associated with posterior circulation stroke. In the past 20 years, with the advancement of interventional technology and the continuous improvement of devices, percutaneous transluminal intervention has gradually been adopted as the preferred treatment for patients with indicated subclavian artery stenosis [1]. The Department of Vascular Surgery of Fudan Zhongshan routinely carries out more than 100 cases of transcatheter intervention in the subclavian artery every year, and the success rate of the operation is as high as 97%, ranking among the best in the country. Today, the editor will share with you a demonstration by the team of Professor Fu Weiguo, Professor Guo Daqiao, and Professor Si Yi from the Department of Vascular Surgery, Zhongshan Hospital, Fudan University, how to use the C-Wave® intravascular shock wave system to successfully treat a complex lesion with severe stenosis of the right subclavian artery opening with calcification.
Case presentation
The patient is an elderly woman, 67 years old. Due to repeated dizziness for many years, he was sent to a local hospital for emergency treatment with sudden dizziness, and the examination showed that the right subclavian artery was stenosis. He tried to undergo right subclavian artery balloon dilation through the radial artery and brachial artery in many places, but failed to perform the attempt due to vascular distortion, and was transferred to the Department of Vascular Surgery of Zhongshan Hospital Affiliated to Fudan University for further diagnosis and treatment.
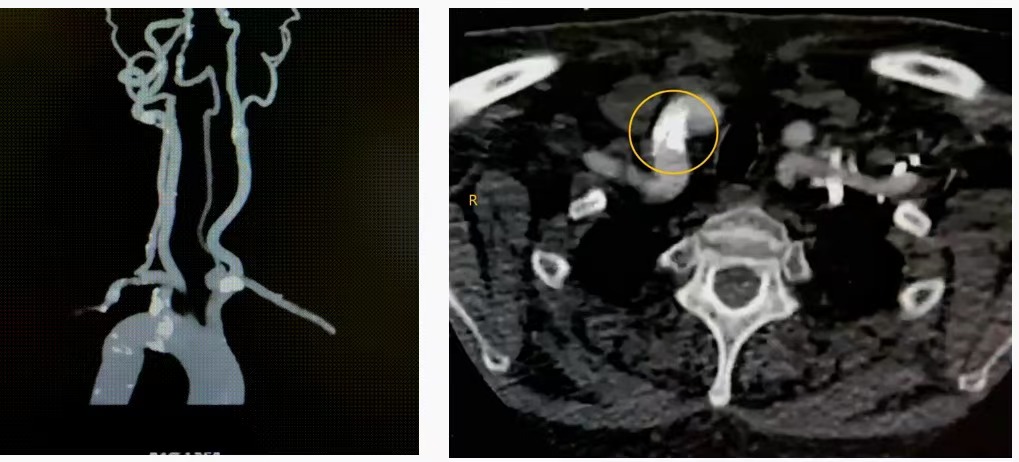
After admission, the examination was completed, and CT showed severe calcified stenosis plaque at the opening of the right subclavian artery and distortion of the subclavian artery.
Diagnosis
Right subclavian artery occlusion with very severe calcification.
Transcatheter subclavian artery stenting is planned.
Surgical procedure
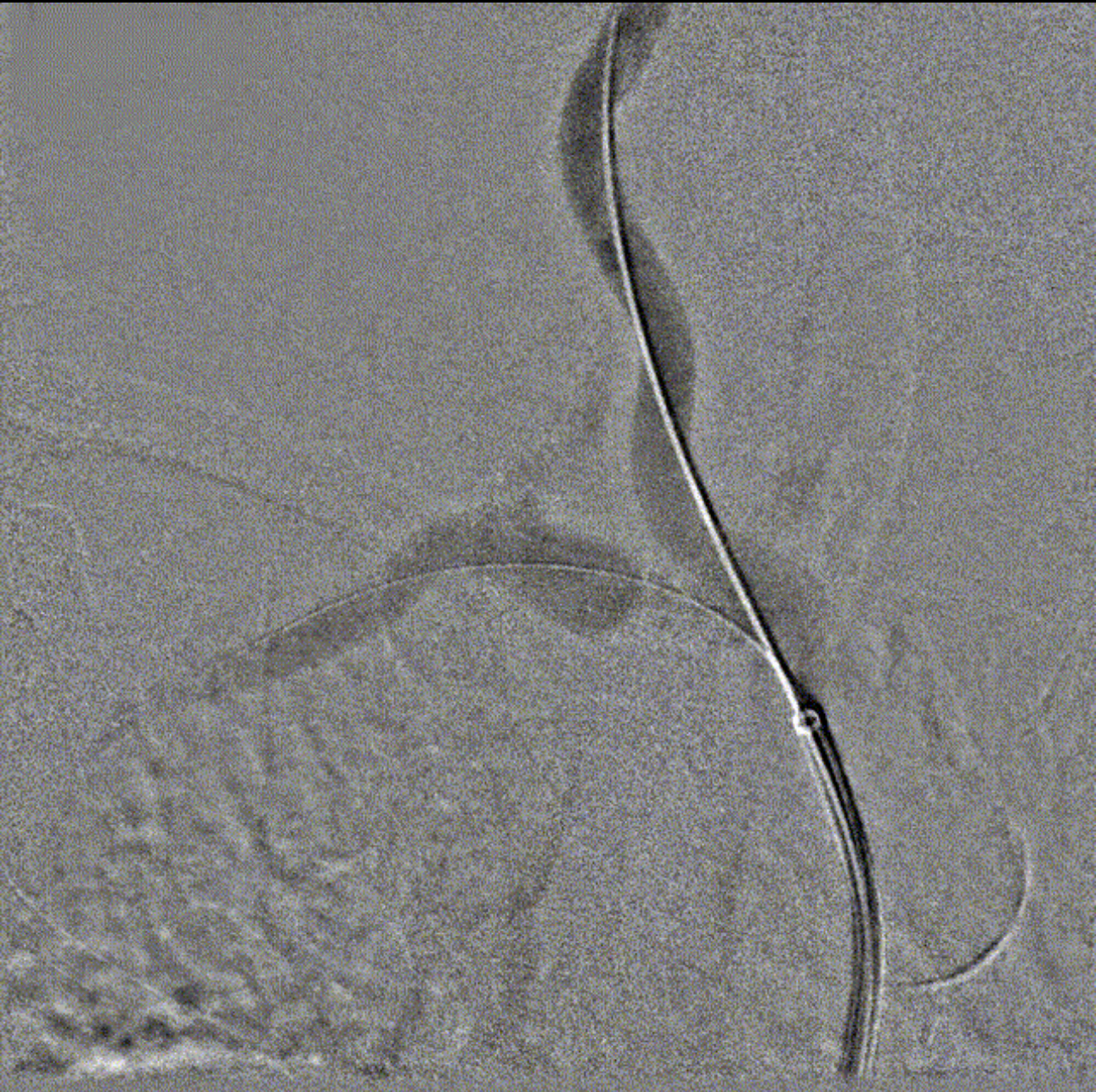
After puncture through the right femoral artery Seldinger method, a 5F catheter sheath was placed, and a 0.035" guidewire (Terumo) and a 4F Pig tube were used to select the ascending aortography, which showed mild stenosis of the left subclavian artery, severe luminal stenosis caused by calcified plaque at the opening of the right subclavian artery, moderate stenosis of the left internal carotid artery ostosis, and reverse blood flow in the right vertebral artery.
Baseline imaging
Difficulty 1: Severe stenosis at the opening of the right clavian artery combined with subclavian artery distortion, and it is necessary to stabilize the approach

The right subclavian artery is twisted and the guidewire pushes with resistance
Countermeasure
Push the guidewire to the distal brachial artery
After "straightening" the blood vessels, the subclavian imaging is repeated to identify the target lesion area
Difficulty 2: Open lesions combined with vascular distortion, the need for support and coordination between instruments
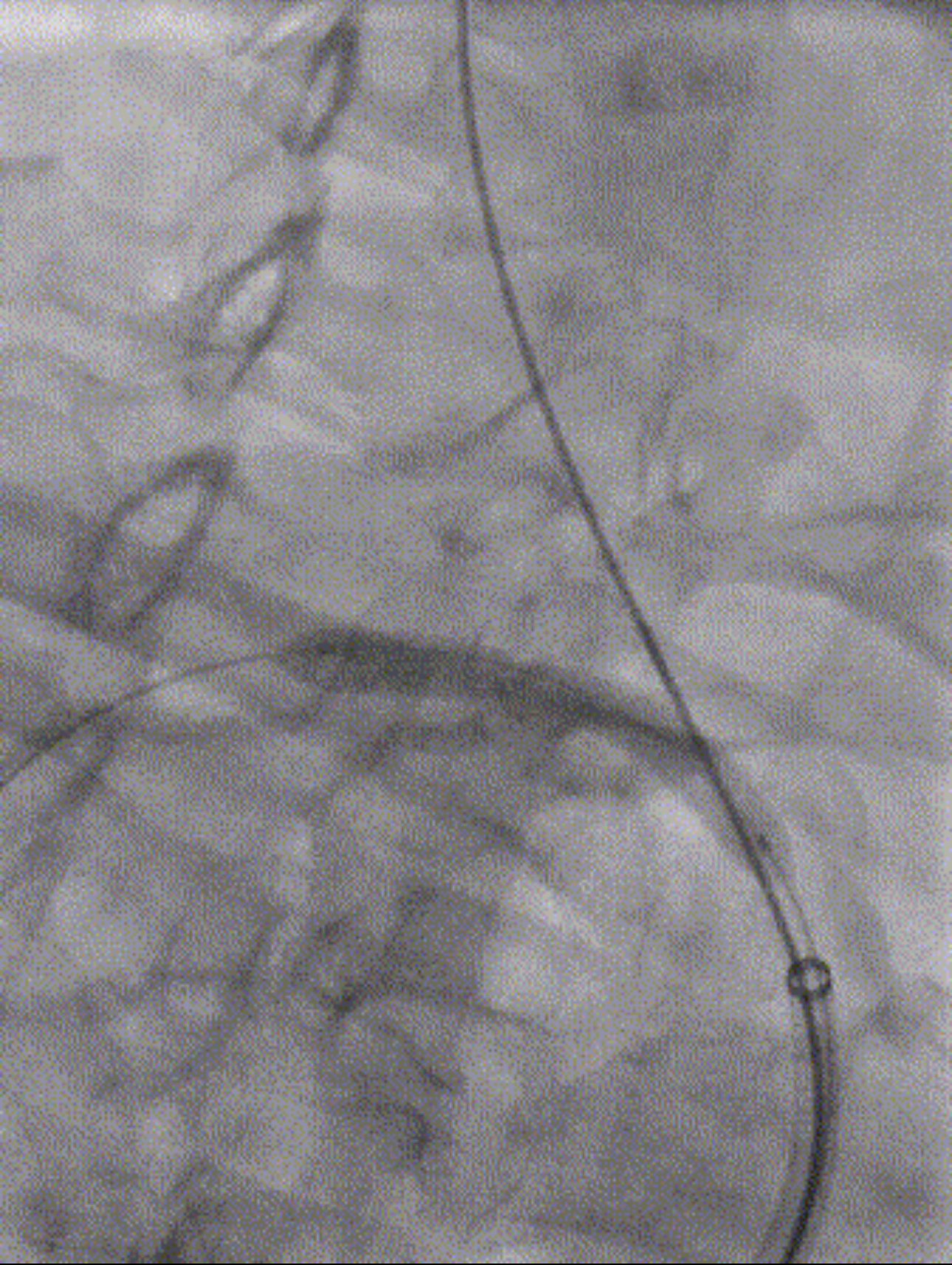
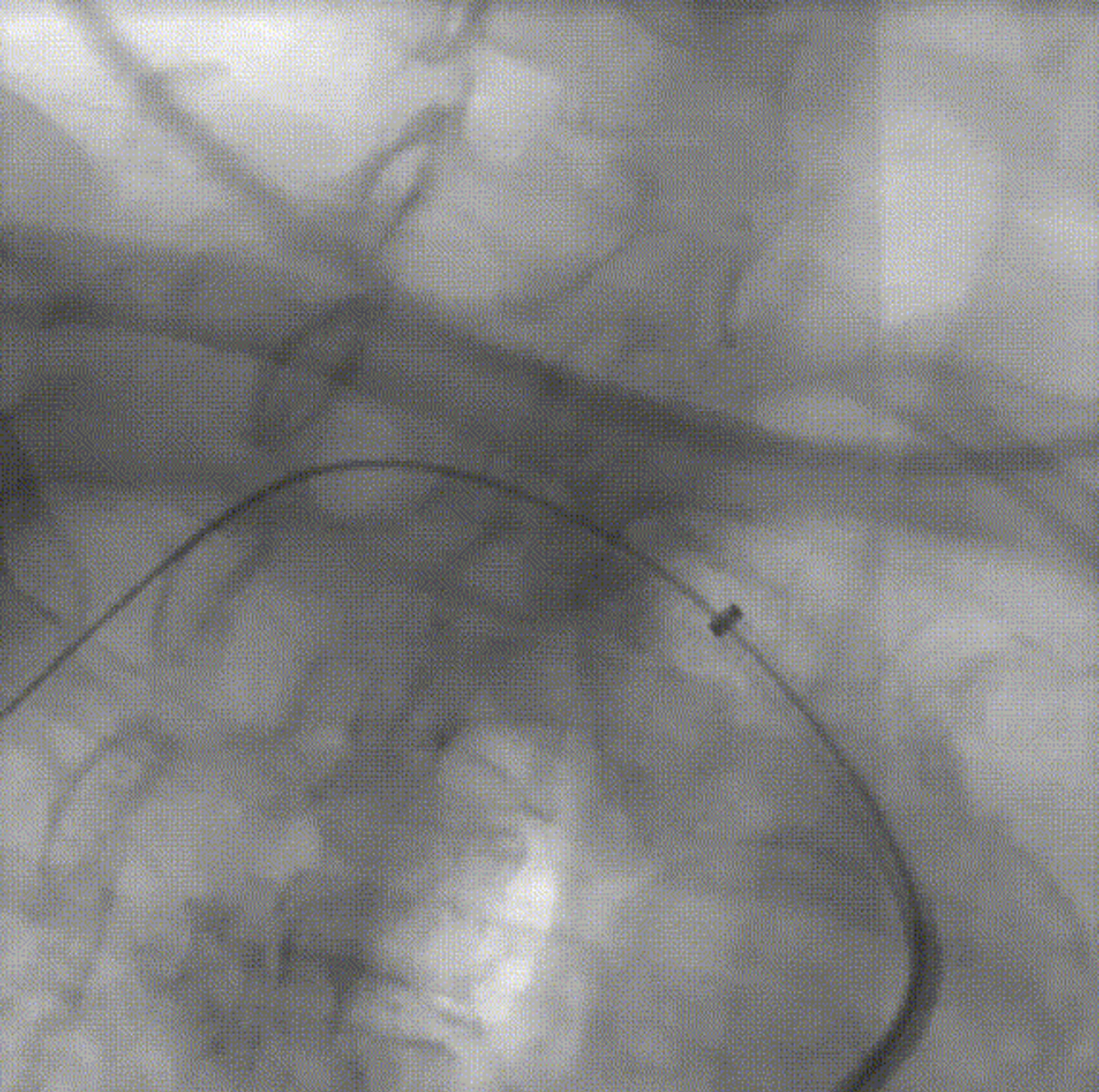
3.0*40mm high-pressure balloon (Mustang, Boston Scientific) pre-dilated lesions
Because the 0.014" guidewire is not as supportive as the hard guidewire, the subclavian artery is twisted, and the shockwave balloon is different from the pre-dilated balloon with better passability, so that the balloon encounters greater resistance when narrowing through the opening
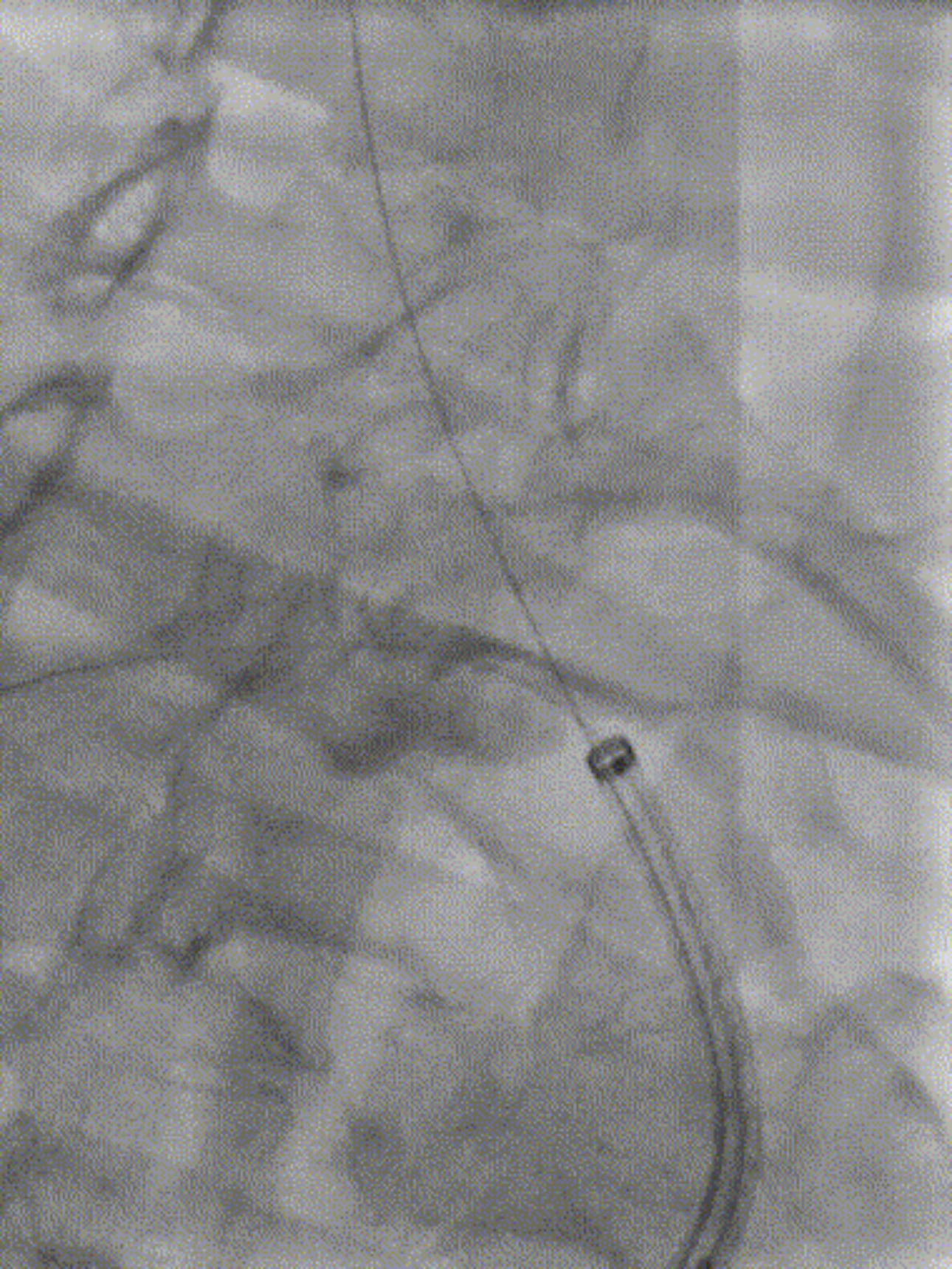
Countermeasure


After the 0.014" guidewire is to the radial artery, another 0.018" guidewire is placed to the right external carotid artery, and the double guidewire technology stabilizes the 8Fr-70 long sheath
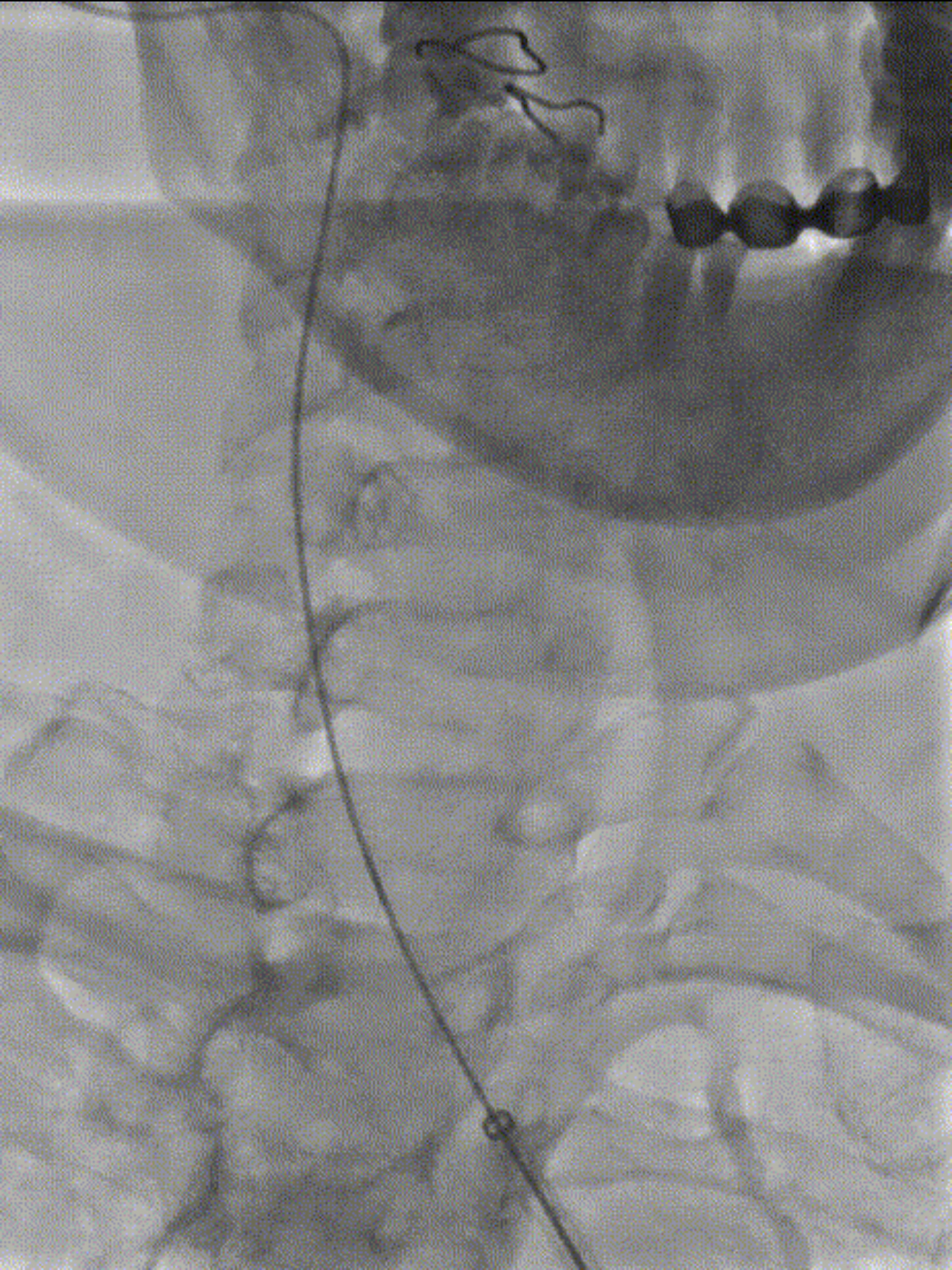
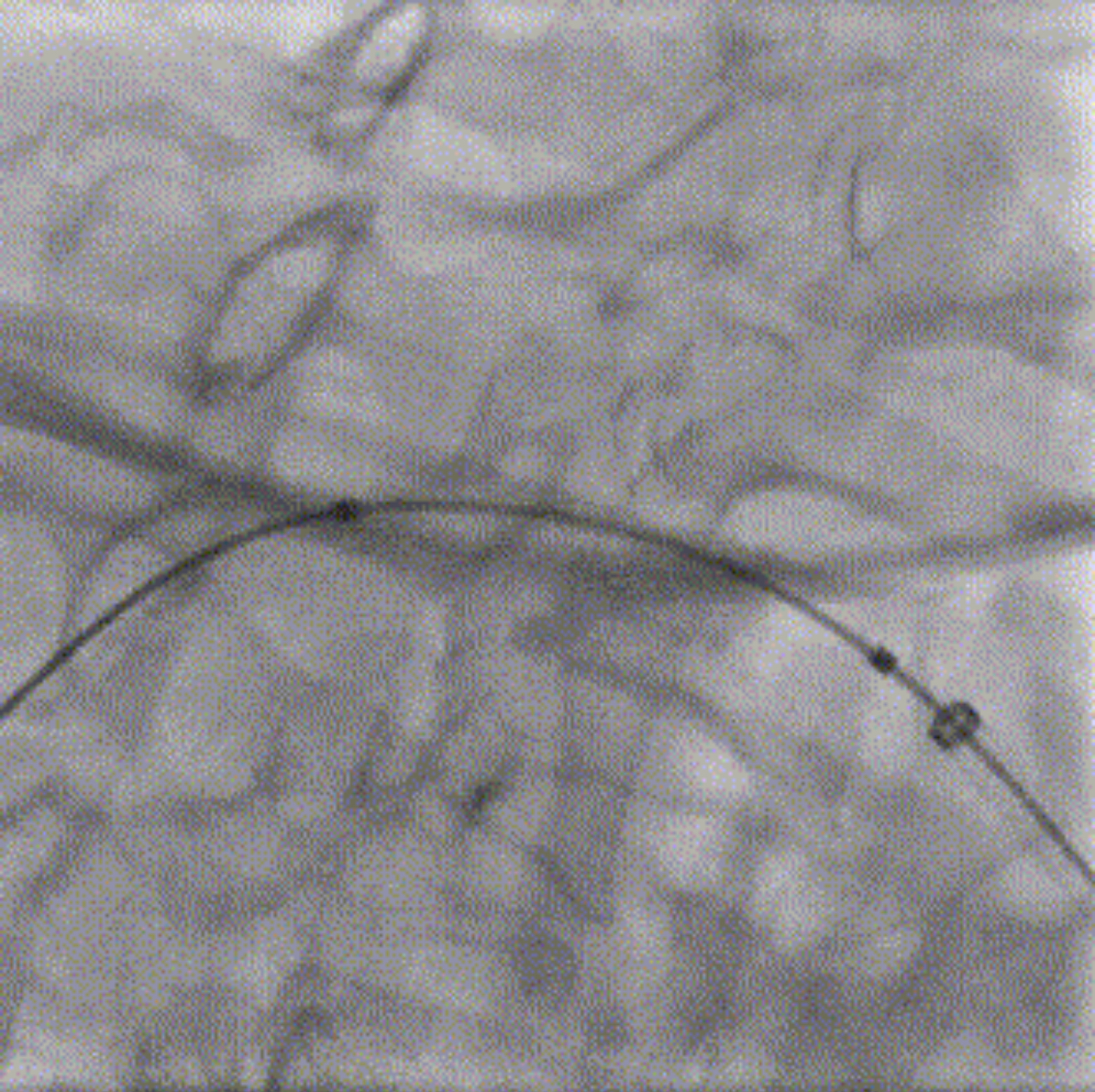
Difficulty 3: Severe eccentric calcification, the need for plaque remodeling
The diameter of the C-Wave® intravascular shock wave balloon (6.5 mm) is smaller than the reference diameter of the target vessel (8.0 mm), which cannot be completely adhered to maximize the energy, and the depth of eccentric plaque crack expansion is limited, and the balloon lumbar sign at 6atm does not completely disappear after 4 cycles (30 times/cycle) of use
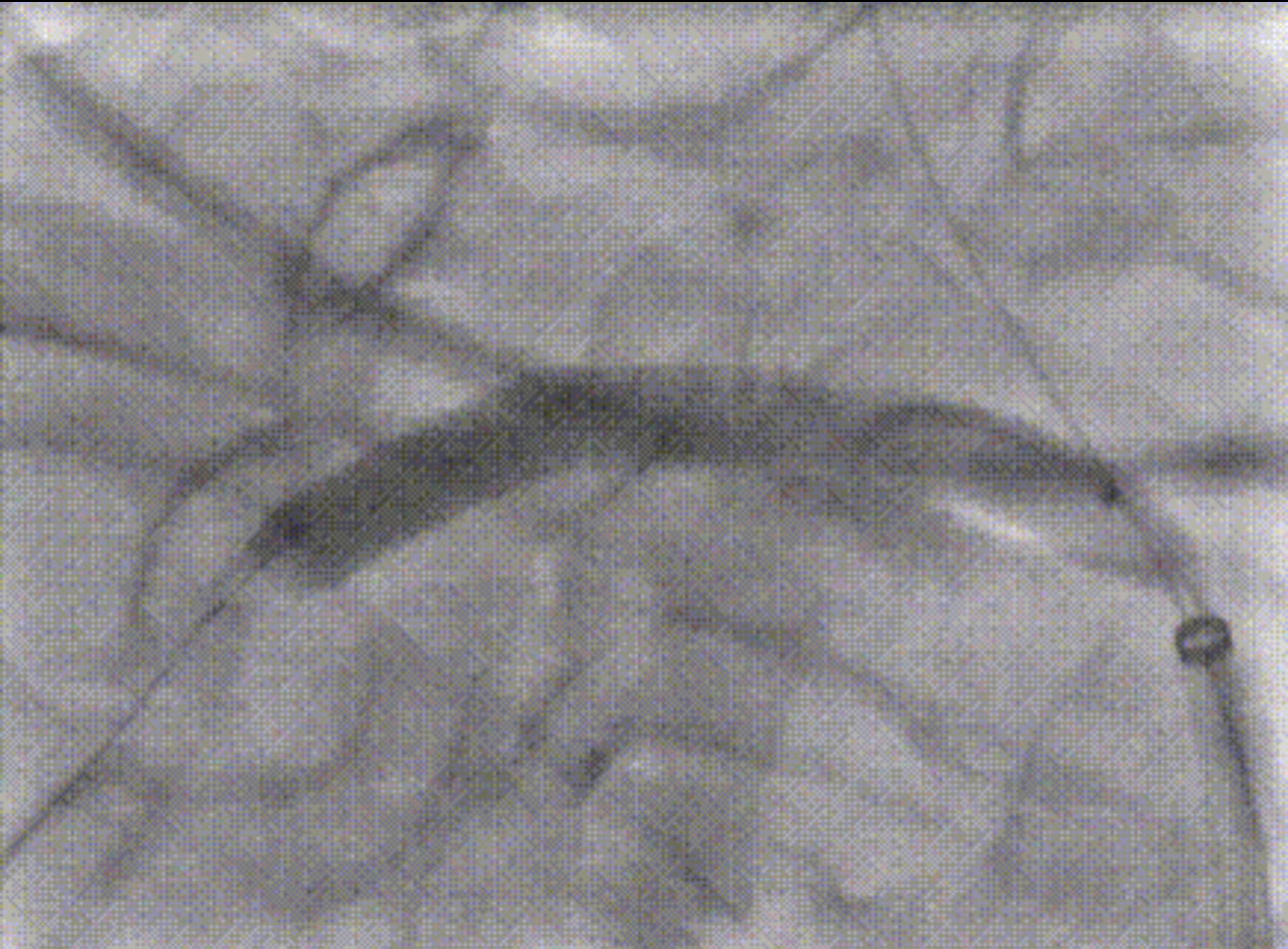
Countermeasure
A 7.0*40mm short high-pressure balloon (Mustang, Boston Scientific) was used to further deepen the fracture and compress the plaque, and a 7.0*40mm drug-coated balloon (ORC, Xianruida) was used and an 8.0*37mm stent (Express LD, Boston Scientific) was implanted, and then the stent adhesion was optimized by 8.0*20mm (Mustang, Boston Scientific).
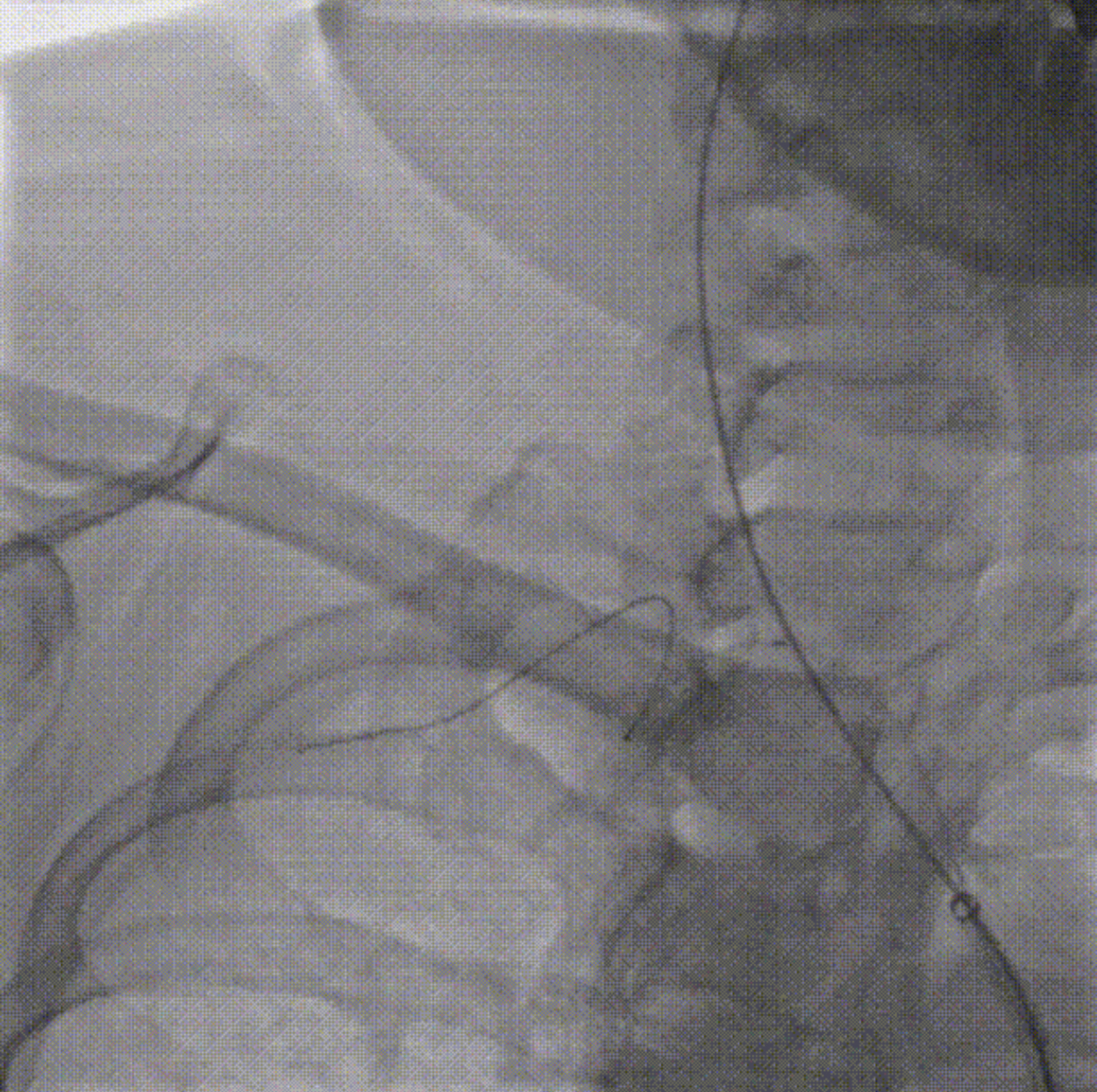
Follow-up imaging showed satisfactory lumen, and blood flow improved significantly compared with before.
One month after the operation, the patient's blood pressure in both upper limbs was unchanged.
C-Wave® Intravascular Shockwave System