
Endovascular repair has been routinely used in the treatment of thoracoabdominal aortic disease, and some patients have too short a distance from the opening of the vital splanchnic branch artery to require revascularization. The fenestration technique is one of the commonly used methods for revascularization, which is divided into in vitro prefenestration and in-situ fenestration. The main difficulties of the extracorporeal fenestration technique are the precise alignment of the window with the target artery, and the stent does not jump forward, move backward, or rotate when the stent is released. The main difficulty of in-situ fenestration is to reach the high-quality window breaking at the fenestration site, i.e. to form the optimal window breaking angle (90°).
The S-wan bipolar adjustable bending sheath is the only sheath with the same plane dual-point bending adjustment function on the domestic market, which can easily adjust the bending angle, stably deliver the instrument to the target target, help doctors improve surgical efficiency and reduce surgical complexity, and easily complete complex actions such as window opening, mountain climbing, and carotid artery overselection.

As a "royal sheath" of fenestration technology, what are the characteristics of S-wan?
S-shaped two-way bend: The S-wan control bend section is composed of the over-selected bend S-bend and the support bend G-bend, forming an S-shaped two-way bend in the cavity;
Superselective: The head end of the S-wan is adjustable from 0 to 270°, and through the curved shape at both ends, it can cope with the overselection of different blood vessel shapes, pipe diameters, endoluminal arteries or carotid arteries, with flexible control performance and high success rate of overselection;
Support: S-wan has its self-developed FREEKNIT variable braiding technology, which provides strong support for passing through the device without rebounding the sheath; At the same time, different supports are carried out through the characteristics of G-bend, vascular morphology, and tube diameter to assist the instrument support after the overselection of complex lesions.

Case 1
Preoperative diagnosis: arterial dissection formation, hypertension grade 2 (very high risk), postoperative state of type A aortic dissection.
Surgical plan: celiac trunk, superior mesenteric artery pseudoluminal embolization + in vitro prefenestration in situ perforation of left renal artery PTA stent + left common femoral artery endarterectomy
Surgical procedure:
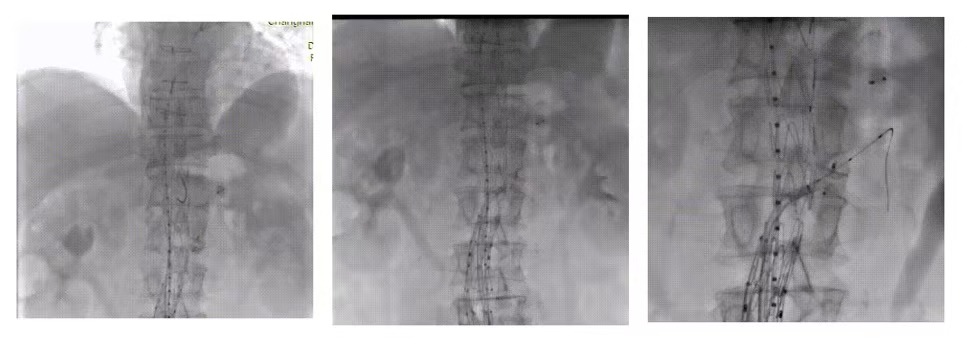
left common femoral artery puncture, embolization of the superior mesenteric artery and celiac dry false lumen respectively and puncture of the right common femoral artery showed that after aortic dissection, the distal false lumen dilation was consistent with the preoperative CTA. Abdominal aortic integrated graft Microport, 20-12-90, was implanted after localization, and marked again after imaging. Thoracic aortic graft Microport on the table, recovered after fenestration at 26-22-160, precise implantation after positioning.
The 8F 55 adjustable bending sheath (Huihe Medical S-wan) was selected, the S-bend angle of the catheter tip was adjusted, and the left renal artery opening was easily aligned to form the best permeabilization angle, and the V18 guidewire and 0.018 support catheter (EV3) were auptured through the window in situ under the strong support of S-wan, and the imaging was confirmed immediately.
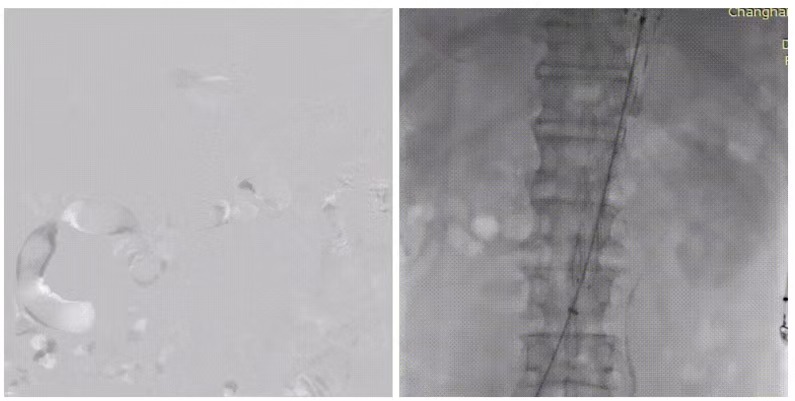
After the 4x80mm balloon was selected, the MPA catheter and 0.035 guidewire were exchanged to superselect the left renal artery opening, and the VBX7x59mm stent was inserted, and the stent position was satisfactory again
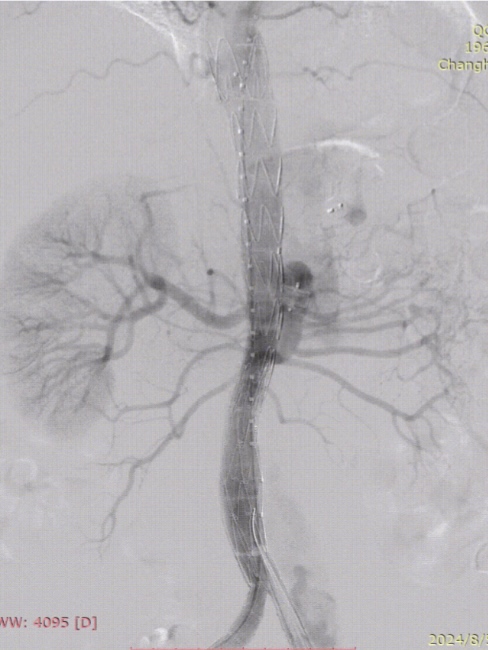
Finally, the aortic dissection was well isolated, and the superior mesenteric artery and both renal arteries were unobstructed.
summary
In this case, the left renal artery was permeated in situ, and the S-wan bipolar adjustable curved sheath was used to establish the best angle for the superselection on the one hand, to ensure the accuracy of the superselection, and on the other hand, to provide stable support for the pre-expansion balloon, the superselection catheter guidewire, and the stent delivery, so that the stent did not jump forward, move backward, or rotate when released, which ensured the safety of the operation and improved the surgical efficiency.
Case 2
Preoperative diagnosis: abdominal aortic dissection, hypertensive disease grade 3 (very high risk), pulmonary nodules, postoperative status of aortic dissection stent implantation
Surgical plan: dissection endovascular isolation + PTA stenting of both renal arteries
Surgical procedure:
puncture of the right common femoral artery, angiography showed distal residual dissection after aortic dissection, right renal artery involvement, and left renal artery opening stenosis, which was consistent with preoperative CTA. Implantation of extracorporeal fenestrated thoracic aortic graft (Microport, 26-22-160)
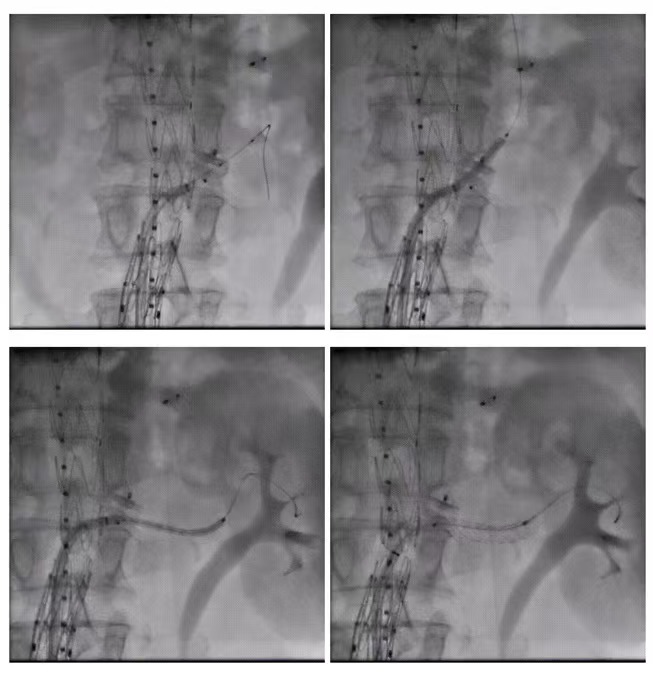
S-wan 8F55 bipolar adjustable curved sheath (Huihe Medical) was selected, first adjusted the sheath to support the G-bend to the appropriate position of the blood vessel wall, and then adjusted the super-selected S-bend to the best angle according to the position of the left renal artery opening, and then introduced the guidewire to cooperate with the MPA catheter to easily and accurately overselect the left renal artery, and after the contrast was confirmed, the PT2 guidewire was exchanged, and the ball diffusion bare stent (Boco, 5X19mm) was introduced to position and release, and the contrast showed that the stent position was satisfactory and the blood flow was smooth.
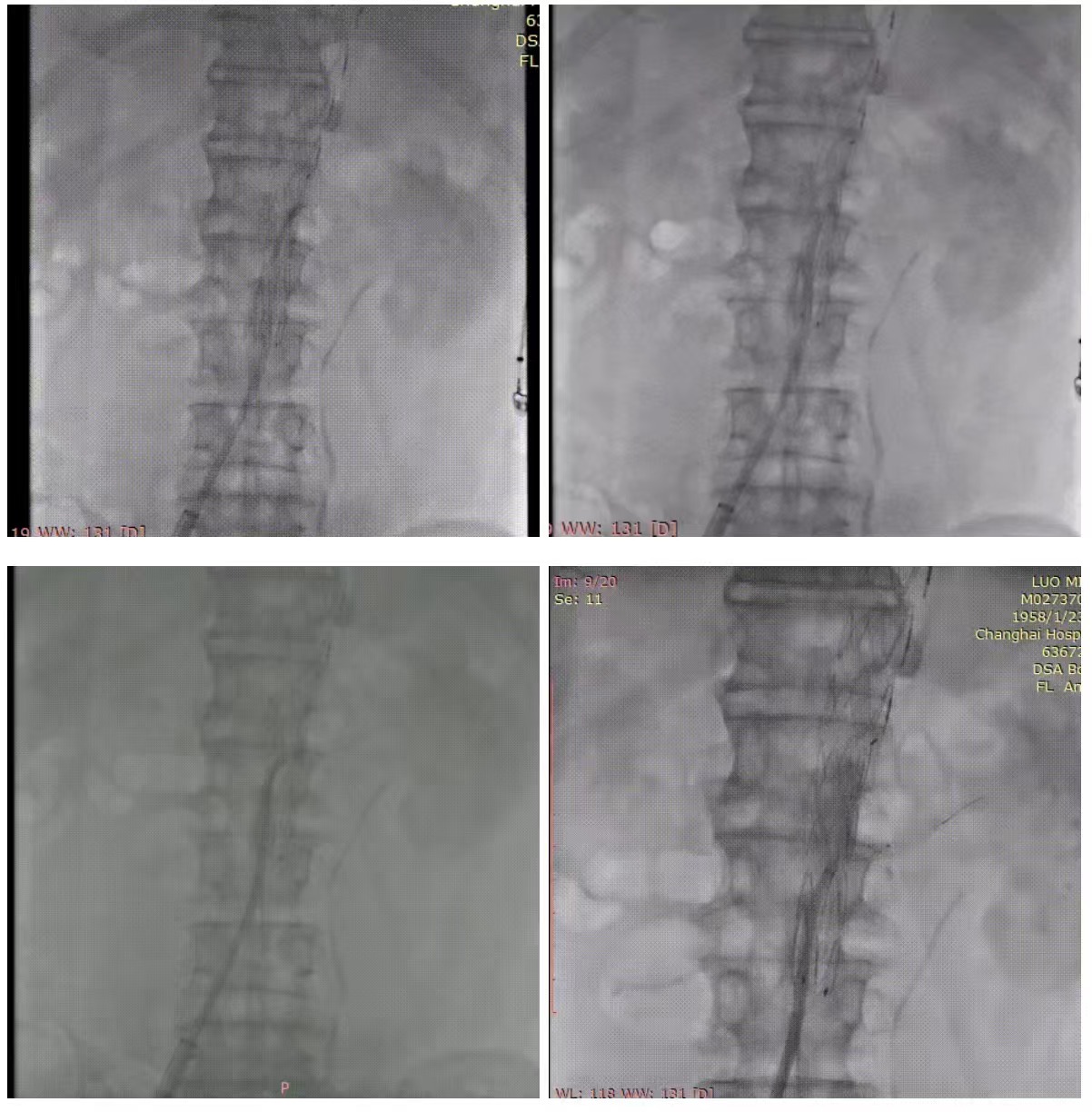
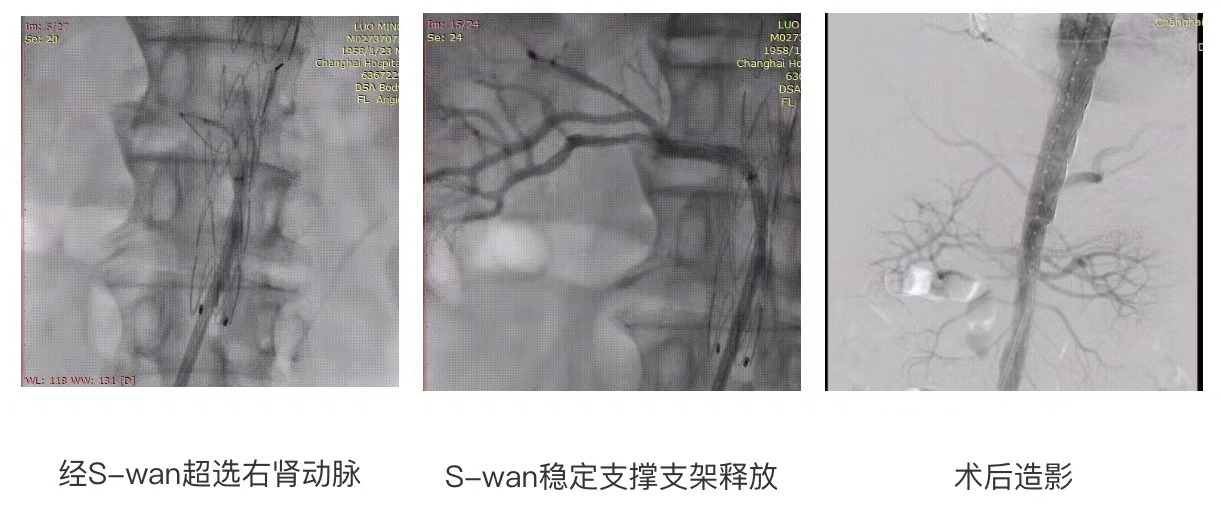
Adjust the S-wan bipolar adjustable curved sheath support bend G bend and overselect S bend to the best angle, lead the V18 guidewire to successfully overselect the right renal artery, after the imaging, the high-pressure balloon was sent through S-wan to dilate the opening of the right renal artery, the VBX (Gore.6x29mm) stent was implanted, and the 10X20mm balloon was used to expand the posteriorly, the instrument passed through the S-wan without rebound, and the contrast showed that the stent was in good position, the celiac trunk, superior mesenteric artery, and both renal arteries were unobstructed, with almost no endoleak, and the right common iliac artery, There is no contrast spillage from the external iliac artery.
summary
In this case, the opening of both renal arteries was stenosis, and the S-wan bipolar adjustable curved sheath was used to support the G-bend and the over-selected S-bend to easily form an S-bend, which formed a precise angle with the renal artery vascular opening, which helped the follow-up catheter to complete the difficult over-selection and provided stable support for stent delivery, which played a role in the success of the operation.
